
OSA vs OHS Key Differences Between Obstructive Sleep Apnea and Obesity Hypoventilation Syndrome
Sleep-related breathing disorders can drastically impair your quality of life, long-term cardiovascular stability, and daily energy levels. Among these conditions, Obstructive Sleep Apnea (OSA) and Obesity Hypoventilation Syndrome (OHS) are two of the most heavily discussed medical diagnoses. Because obesity is a prominent risk factor for both, they are frequently confused or misdiagnosed. However, treating them requires distinct medical strategies.
At Respiratory Store & Sleep Solution, we believe that understanding the exact pathology of your condition is the first step toward effective management. In this guide, we break down the definitive OSA vs OHS differences, their symptoms, diagnostic guidelines, and ideal therapy options.
The Core Medical Mechanisms: What Happens Inside?
To understand how these conditions differ, we have to look at how they affect the body’s respiratory system during sleep versus wakefulness.
1. Obstructive Sleep Apnea (OSA)
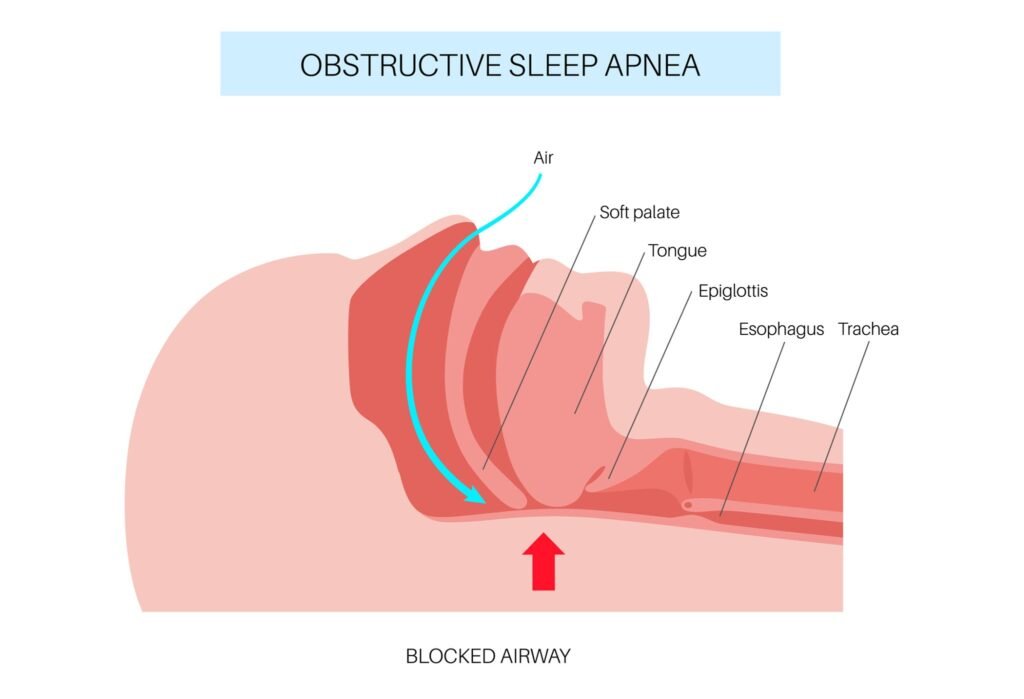
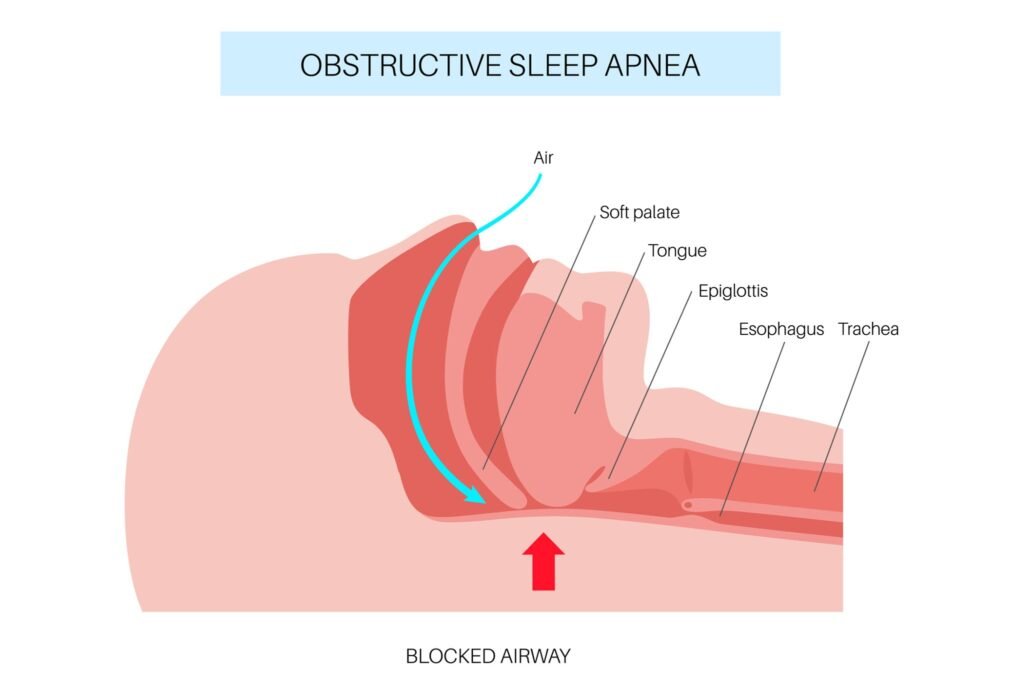
OSA is purely an anatomical, mechanical issue. When a patient goes to sleep, the muscles in the back of the throat relax. In individuals with OSA, this relaxation causes the soft palate, tonsils, or tongue to collapse backward, physically sealing off the trachea (windpipe).
As shown in the diagram above, this blocked airway cuts off the flow of oxygen completely (apnea) or partially (hypopnea) until the brain triggers a brief, unconscious micro-arousal to restart breathing. Crucially, people with isolated OSA have entirely normal breathing and healthy blood gas levels when they are awake.
2. Obesity Hypoventilation Syndrome (OHS)
OHS—historically referred to as Pickwickian syndrome—is a much broader, systemic respiratory failure. It occurs in individuals with severe obesity (typically a Body Mass Index or BMI greater than 30). In OHS, the sheer physical weight of excess fat tissue on the chest wall and abdomen acts as a restrictive restriction, squashing the lungs and preventing them from expanding fully.
Unlike OSA, this is a 24/7 issue. Because the lungs cannot take deep breaths, the body experiences continuous alveolar hypoventilation mechanism issues. This means the lungs fail to exhale enough carbon dioxide ($CO_2$), leading to a dangerous buildup known as chronic carbon dioxide retention in the blood, alongside persistently low oxygen levels, even while wide awake.
Side-by-Side Comparison: OSA vs OHS
| Diagnostic Parameter | Obstructive Sleep Apnea (OSA) | Obesity Hypoventilation Syndrome (OHS) |
| Primary Structural Defect | Upper airway collapse (Throat block) | Chest wall restriction (Heavy chest) & faulty brain respiratory drive |
| Awake Blood Gas Status | Completely normal oxygen ($O_2$) & carbon dioxide ($CO_2$) levels | Daytime hypercapnia (High $CO_2$) and awake chronic hypoxemia (Low $O_2$) |
| Body Mass Index (BMI) | Can affect any weight profile (lean or obese) | Strictly linked to a BMI greater than 30 |
| Diagnostic Pathway | Standard polysomnography sleep study | Sleep study + arterial blood gas test (ABG) |
| Primary Device Line | Auto-CPAP / Standard CPAP | Advanced BiPAP or Non-invasive ventilation medical devices |
Recognizing the Overlapping and Distinct Symptoms
Because these two conditions frequently coexist—with up to 90% of OHS patients also suffering from severe OSA—the overlapping clinical signs can blur the lines during an initial visit to a sleep disorder clinic Lahore or other healthcare facilities.
Common Shared Features:
- Loud, disruptive snoring with choking or gasping sounds at night.
- Severe daytime sleepiness due to fragmented sleep patterns.
- Morning headaches and dry mouth upon waking.
Distinct Symptoms That Signal OHS:
Because OHS introduces chronic carbon dioxide retention, it causes unique systemic signs that are absent in isolated sleep apnea breathing disorders:
- Severe Daytime Lethargy: The constant toxicity of high blood $CO_2$ causes profound, unrelenting fatigue that makes patients fall asleep mid-conversation or while eating.
- Cyanosis: A distinct bluish tint on the lips, fingernails, or skin due to persistent nocturnal hypoxemia diagnostic states carrying over into awake hours.
- Right-Sided Heart Failure (Cor Pulmonale): Chronic lung restriction forces the right side of the heart to work harder to pump blood through narrow lung vessels, leading to noticeable swelling (edema) in the legs, ankles, and feet.
How Pulmonologists Diagnostic Each Condition
A specialized pulmonologist cannot differentiate between these conditions using an visual assessment alone. A detailed clinical pathway must be deployed:
- Polysomnography Sleep Study: This tracking monitors airflow, chest effort, and drops in blood oxygen saturation overnight. It quantifies the severity of blockages.
- Arterial Blood Gas Test (ABG): This is the definitive dividing line. An ABG draws blood directly from an artery to measure the partial pressure of carbon dioxide ($PaCO_2$). If the awake $PaCO_2$ is greater than $45\ mmHg$, it confirms daytime hypercapnia, confirming an OHS diagnosis.
Tailored Treatment Pathways at Respiratory Store & Sleep Solution
Because their biological origins differ, the equipment setup required to treat them successfully must be carefully calibrated.
Managing OSA with CPAP Therapy
For standard Obstructive Sleep Apnea Pakistan cases, a Continuous Positive Airway Pressure (CPAP) device is the gold standard. It acts as an invisible air splint, keeping the upper airway open. You can browse our customized setups on our CPAP rental and pricing directory to see available choices.
Managing OHS with Advanced BiPAP / NIV Therapy
Standard CPAP often fails for OHS patients because it only keeps the throat open; it doesn’t help the exhausted chest muscles expand to push out heavy carbon dioxide. Therefore, doctors prescribe a Bilevel Positive Airway Pressure (BiPAP) system or advanced non-invasive ventilation medical devices.
BiPAP offers two distinct pressures: a higher IPAP (Inspiratory Positive Airway Pressure) to actively assist the lungs in breathing in, and a lower EPAP (Expiratory Positive Airway Pressure) to keep the airway stable. As a premier ResMed BiPAP supplier Pakistan, our technical experts configure specialized breath-timing features that guarantee carbon dioxide is flushed out safely. For more information on device options, view our comprehensive BiPAP and non-invasive ventilator product catalog.
Conclusion: Getting the Right Device for Your Lungs
While both conditions threaten your respiratory health, knowing whether your challenge lies in an upper airway blockage (OSA) or a deep-seated chest restriction with gas imbalance (OHS) changes your entire management protocol.
If you or a loved one are struggling with severe daytime exhaustion, morning headaches, or low oxygen profiles, do not wait for complications to escalate. Respiratory Store & Sleep Solution is fully equipped to deliver, calibrate, and monitor premium, certified equipment tailored exactly to your clinical diagnostics. Reach out to our specialized care coordinators through our contact and consultation page to safeguard your breathing today.
Frequently Asked Questions (FAQs)
Q1: Can someone have both OSA and OHS at the exact same time?
Yes. This clinical combination is frequently called “Overlap Syndrome.” In fact, the vast majority of individuals diagnosed with Obesity Hypoventilation Syndrome care requirements also present with severe obstructive blockages during their initial polysomnography sleep study.
Q2: Why is a standard CPAP machine sometimes insufficient for treating OHS?
A CPAP machine provides one constant pressure level to hold open a collapsed throat. It lacks the dual-pressure mechanical support needed to alleviate the workload of a heavy chest wall, which is essential for correcting daytime carbon dioxide imbalances.
Q3: Is Obesity Hypoventilation Syndrome reversible?
Yes, significant and sustained weight loss (either through controlled medical metabolic strategies, lifestyle changes, or bariatric surgery) can reduce chest wall restriction, allowing blood gas parameters to return to normal levels. However, temporary BiPAP respiratory support is vital while losing weight.
Q4: What are the dangers of leaving OHS untreated?
Untreated OHS can lead to severe medical issues, including pulmonary hypertension (high blood pressure in the lung arteries), severe right-sided heart failure, cognitive deficits due to lack of oxygen, and life-threatening respiratory failure requiring emergency ICU placement.
Q5: How can I arrange an in-home trial for a BiPAP machine in Lahore or Islamabad?
You can easily coordinate an active home setup by visiting our specialized location branches. For local services, check our Lahore main showroom location or our twin-cities Rent CPAP machine Islamabad portal to schedule a technician visit.